
It's been five months since writing about our experience on the other side of medicine as patients. Today I want to fill the gap between my last post and the present day.
Last I wrote, Chloe was starting prednisone 7.5mg BID x 7 days for her thrombocytopenia. Having the crushed form was much easier than the oral suspension. If you have kiddos needing prednisone, go for the pills and crush them.
After finishing our course, we discovered that her platelet counts remained at 7,000. Because of this, on July 25th, we decided to start her on Nplate, which was titrated weekly by 1 mcg/kg until reaching the max dose of 10 mcg/kg.
Nplate is a TPO receptor agonist and is given as a subcutaneous injection. This medication stimulates the bone marrow to produce more platelets. The hope was for Chloe to produce more platelets than are destroyed to elevate her counts. But, just like previous medications, this is not a cure.
This medication required us to go to the hematologist every week to check her platelet counts and to administer the injection (as we had to continue to titrate).
We reached the max dose on October 20th. Throughout the three months, there wasn't any change in her platelet count (she stayed in the 2,000 - 7,000 range).
It's worth mentioning that although there wasn't a change in platelet count, she was asymptomatic. No bruising, petechia, epistaxis, wet purpura, or rectal bleeding. So there was clinical improvement despite her lab results. During the last week on Nplate, however, we noticed that the symptoms began to recur.
On October 31st, we stopped the Nplate and started her on Promacta (which she is still currently on). Like Nplate, her counts have not improved, but she has no clinical evidence of bleeding. The difference is that this medication has made her jaundice (a benign side effect of this medication). However, we did our due diligence and ruled out hepatic injury and hemolysis.
Finally, on November 7th, we had our first rheumatology appointment.
There are three main reasons we wanted to see a rheumatologist:
Chloe developed a malar rash starting at 2 months of age. I brought it to the attention of her pediatrician and hematologist, but I was told it didn't resemble the classic butterfly rash in lupus. There also aren't any case reports of SLE starting that young (excluding neonatal lupus), so it made it highly unlikely to be SLE. But her rash persists, and I still have some doubts.
As a side note, I did notice a couple of painless oral ulcers back in August. I happen to look inside her mouth at the time they were present.
She's young. Bleeding symptoms began at 5 months of age, and she was diagnosed at 6 months of age. The peak incidence of ITP is usually between 2-5 years of age.
She's refractory to treatment, failing IVIG, prednisone, NPlate, and currently promacta.
We were evaluated by rheumatology and were told that we didn't need a follow-up appointment as there weren't any red flags. But, if any abnormalities were seen in the lab results, we would be scheduled to return.
I also wanted to rule out a primary immunodeficiency disorder as the underlying cause. So, we were referred to immunology to rule that out.
Her initial labs returned abnormal, prompting a more in-depth workup. Because of her weight, we had the maximum blood drawn weekly for three weeks.
Chloe goes to every single visit with a massive smile on her face. She waves hello and says goodbye to the staff. This demeanor doesn't change during blood draw either. In fact, during her last appointment, she was getting blood taken from her left arm as she reached to grab a snack with her right arm.
She has her very own fan club in the heme/onc clinic. It truly amazes me to see how happy, calm and collected she is throughout this entire journey. It lets me know that she feels safe and loved. This has always been our goal as parents.
Pertinent lab results returned as follows:
ANA titer positive: 1:40 with speckled pattern
Elevated anti-dsDNA antibody IgG: 101 IntlUnit/mL (positive >75)
Negative anti-Sm, anti-U1 RNP, SCL-70, SSA, SSB antibodies
Positive B2 GLYCOPROTEIN-1 AB IgG: 90 SGU (positive > 20)
IgM/IgA negative
Lupus anticoagulant and anticardiolipin antibodies were negative
Low C3 (78 mg/dL)
C4 was normal
CH50 and AH50 levels normal
She's had her immunoglobulins checked twice now:
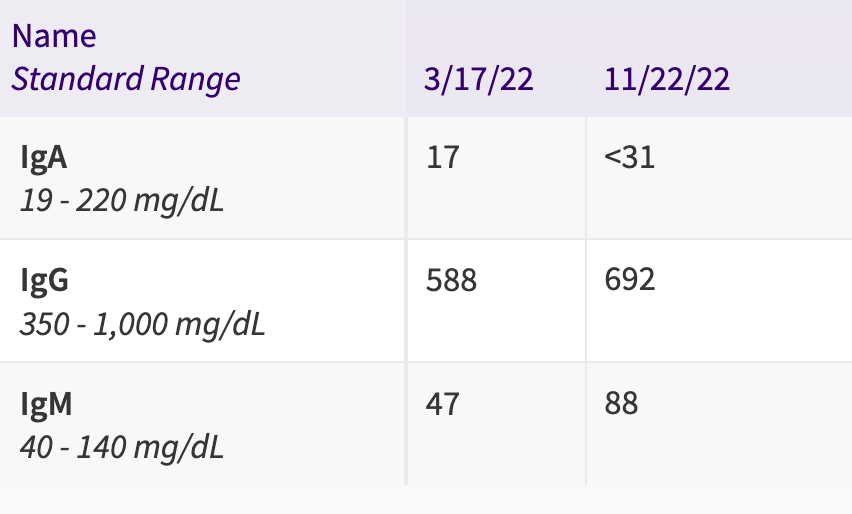
As you can see, IgG and IgM were normal. But we still need to get a value for our most recent IgA level, as it was reported as <31 (which isn't helpful). We need to clarify this, as selective IgA deficiency is associated with autoimmune disease and antibody production.
It's important to note that immunoglobulin levels can fluctuate until a child is four years old. Therefore a definitive diagnosis of selective IgA deficiency can't be made until then.
T/B cell lymphocyte and genetic thrombocytopenia panel results are still pending. We drew vaccine titers, but it’s worth noting Chloe hasn’t had any vaccinations after her fourth-month physical due to her thrombocytopenia, so these will invariably be low.
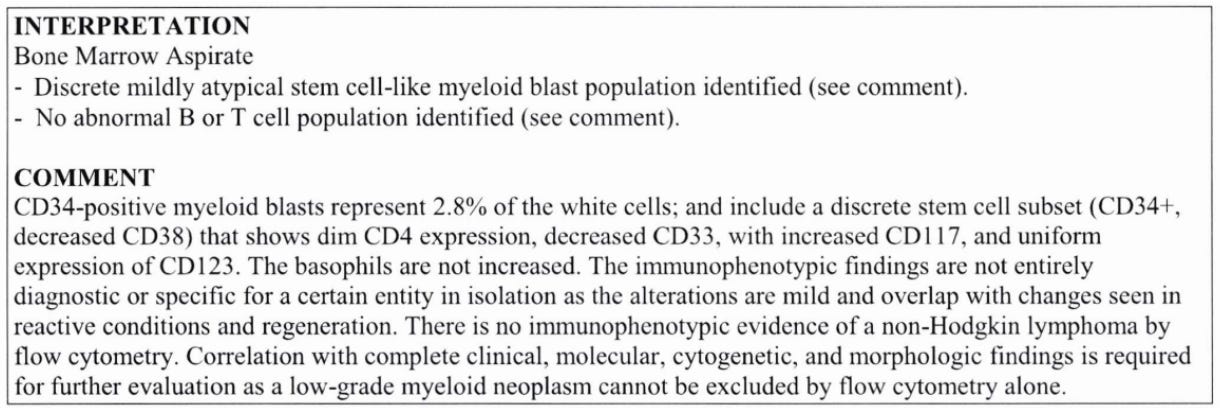
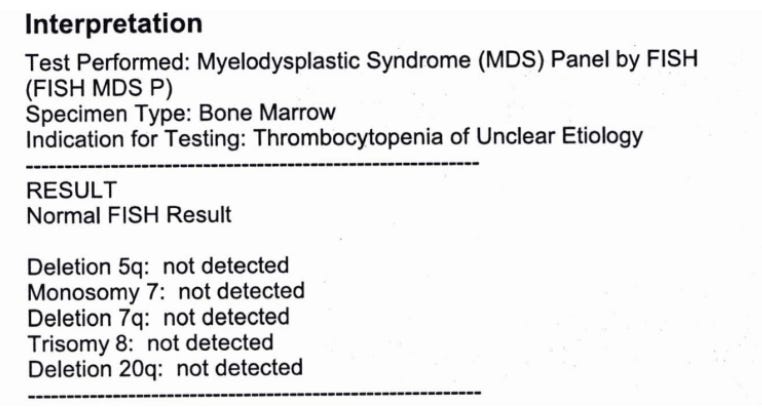
We reached out to Mayo Clinic in Rochester, Minnesota, to get another set of eyes on her labs. The physician we spoke to recommended we get genetics to consult as well (so we are). They also want us to have the bone marrow biopsy repeated in June 2023 (one year after the initial sample) due to her initial bone marrow result:
The repeated bone marrow makes us a little nervous as she had an adverse reaction the first time. The anesthesiologist informed us that she wasn’t staying sedating with the propofol. Because they couldn’t increase the dose further, they added ketamine. At that point, our little girl stopped breathing. They had to bag her for 20 seconds until she started breathing on her own again. At the time, she was only 6 months old, but as a parent, it still makes us nervous thinking about repeating this procedure.
The plan is to finish the evaluation to figure out the next steps. Before starting any medication that could skew lab results (i.e., rituximab), we want to understand what we're dealing with.
At this point, we haven’t heard from the rheumatology physician in three weeks, even as we start to see specific abnormalities in our daughter’s lab results.
For those in practice, always remember patients are people, not just a set of labs. Their lives continue even after they leave your office. As clinicians, we’re so focused on morbidity and mortality that we often forget what patients go through between visits.
Typical concerns can turn into worst-case scenarios.
Keep the empathy alive, my friends.
Praying for you and family! May God bless your little girl in every step of the way!
What a tough journey you and your family are going through Andrew! Our thoughts and prayers are with you all. Hoping you find some answers and guidance for sweet Chloe!